Open Data for Developing Economies Case Studies
Uganda’s iParticipate
Open Data for Achieving Better Health Outcomes
by Michael P. Canares, Andrew Young and Stefaan Verhulst
Problem Focus / Country Context
According to the World Health Organization (WHO), Uganda has among the worst health service delivery provisions in the world, resulting in poor health outcomes for its citizens. The country has among the lowest life expectancy (54 years in 2015) and highest mortality rates (344 in 2013) in the world.4 As of 2015, one in every 300 births ends a mother’s life, and one of every 30 children born will not be able to survive beyond one year.5 Communicable diseases, especially tuberculosis, claim the largest portion of lives in the country. HIV prevalenceis high, with at least 1.5 million people affected, and the country is among those with the highest new cases of HIV/AIDS globally.6
Several factors contribute to such poor health outcomes. First, there is a serious dearth of health workers who can attend to the needs of a growing population. A recent study pointed, for instance, to the very low ratio of health care providers to population in the country, coupled and aggravated by an insufficient budget.7 Most medical personnel are concentrated in urban areas, to the disadvantage of patients in rural areas. Another problem is pervasive corruption in the health service sector—manifested in a variety of ways, including paid workers failing to arrive at work on time with no fear of repercussion8 and the misappropriation of public funds for construction of health service facilities.9
A lack of data also hampers the quality of service delivery. Studies point in particular to a shortage of data related to disease prevalence,10 service delivery indicators, and health outcomes.11 While some forms of health data are collected, these are largely in paper formats and not shared publicly. The Ugandan Ministry of Health Website,12 which is supposedly the repository of publicly accessible data on health in the country, publishes all information as PDF files. The data is often insufficiently granular to contribute to useful analysis and access to much information, including health human resource data, is often restricted.
Open Data in Uganda
According to the 2015 Open Data Barometer,13 Uganda ranked 70th out of 92 countries surveyed. The government has made some efforts to use information technology and e-government practices to improve the delivery of public services. In addition, several of its ministries, especially health, environment, and national statistics, have practiced proactive disclosure of data online, though in separate, unlinked websites, and in incompatible formats that make the data difficult to use.
In 2015, the World Bank report on open data readiness in Uganda14 emphasized that while the country is well-positioned to implement an open data initiative, its ability to actually do so will depend on several issues related to policy, data capacity, and civic engagement. To date, there is no policy which mandates disclosure of government data and protects privacy. In addition, there is a definite lack of technology skills on the part of government employees. Citizens are also limited in their ability to access data by poor broadband access and low data literacy.
A review15 funded by the Indigo Trust, a funding organization focused on transparency and accountability in Sub-Saharan Africa, found that there exist more than 10 data disclosure mechanisms within the Ugandan government, but that these cover only a few government agencies, namely public finance, water and environment and national statistics. The absence of a centralized open government data portal prompted several actors to publish data relevant to Ugandan governance and public life in different portals like data.ug (supported by UNICEF), uganda.opendataforafrica.org (supported by the African Development Bank) and several other sector-focused initiatives initiated by civil society organizations, international agencies, and academia. The tendency of actors from non-governmental sectors to step up to fill open data gaps left by governments is a common theme across this series of case studies.
Data Collection and Disclosure in the Ugandan Health Care System
Uganda’s Ministry of Health is responsible for one of the important sectors in the country. Its primary mandate is to formulate policies related to health, manage partnerships, resource mobilization, capacity building, and quality control on health service delivery, as well as to monitor and evaluate overall health sector performance across the country and at every level of government.
Health care provision in Uganda is undertaken by both public and private actors. Public health service providers have a decentralized structure which consists of national referral hospitals, semi-autonomous regional referral hospitals, and a well-established District Health System under the leadership of the District Directorate of Health Services in each of the country’s 111 districts. The intent behind decentralization was to make services reach even the most remote communities, and health centers in the country are broken up into four categories (ranging from the most rudimentary facilities, Health Center 1, to the more advanced, Health Center 4). Health service delivery is based on a referral system, with cases escalated up the categories depending on their level of complexity and facilities required.
Private sector health service provision is offered by a number of actors. These include facility-based private providers, not for profit (PNFP) providers, non-facility based PNFPs, private health practitioners, and traditional medical service providers. Facility-based PNFPs are those who own or operate their own hospitals and clinics; an example of a non-facility based PNFP would be an NGO offering medical services. Private health practitioners refer to those that provide primary and secondary level health services and include a wide range of actors, such as diagnostic centers, private medical and dental clinics, and pharmacies.
The capacity of Ugandans to seek treatment from private sector health service providers, without having to go through the long process of referral in the government system, is affected by their financial capacity and geographic location. In some areas, especially in rural Uganda, there are no private PNFPs or private health practitioners. For residents of these areas, many of whom also lack the financial capacity to pay for private health care, government health centers are the only option (they may also submit themselves for treatment to traditional herbalists or other “informal” healers without formal training).
The government collects health care data from both the public and private sectors (though it does not collect information from the informal sector). The data collected is largely stored in paper-based formats,16 based on a set of standardized forms issued by the Ministry of Health (MoH). Aggregation of data is done at the level of MOH, through a Health Management Information System (HMIS17) which aims to ensure timely aggregation, storage and retrieval of health information. Data quality is largely (and often negatively) affected by the capacity of lower-level administrative agencies to collect and report data in an effective manner. As a WHO report puts it: “lower administrative levels chronically lack the capacity to capture and report vital events such as community births and deaths.”18 Another study19 reported that data collected regarding inpatient, outpatient, and health coverage indicators was less than 85 percent complete.
The MOH has made several noteworthy attempts to address these issues. For example, in 2010 the MOH launched the Human Resource for Health Information System (HRHIS),20 a database platform developed in partnership with USAID that paved the way for comprehensively identifying staffing gaps down to the district level. The MOH has also sought to address data shortcomings by increasing the budget for human resources in public health centers.21 Despite improvements, however, most of the data collected is not available to the public, and even when available, is difficult for ordinary citizens to understand. HMIS data, for example, requires registration for access and is available only to authorized users through a dashboard. HRHIS data, on the other hand, can be downloaded in spreadsheets format, but needs a trained user for the spreadsheets to be understood.
Key Actors
Key Data Providers
Government of Colombia
The Ugandan government, through different portals, makes accessible the majority of data used for iParticipate. In particular, open data provided through the portal by the Ministry of Health plays an important enabling role. The project also leverages some limited data from private sector health providers, demonstrating the potential for more cross-sector data collaborative arrangements.
Key Data Users and Intermediaries
Established under the United Kingdom Department for International Development-funded Catalysing Access to Information and Communications Technologies in Africa (CATIA) initiative, the Collaboration on International ICT Policy in East and Southern Africa (CIPESA) is a civil society organization that “facilitates the use of ICT in support of development and poverty reduction.”22 CIPESA’s iParticipate project was established with funding from the Swedish Program for ICT in Developing Regions (SPIDER), a resource center working across sectors to leverage ICTs for development purposes. SPIDER, in particular, seeks to enable “the collaboration and sharing of experience between different actors in the field to reach better development results.”23
Intended Beneficiaries
The iParticipate initiative aims to catalyze the use of ICT in citizen’s engagement and participation in governance.24 The project intends to build the capacity primarily of journalists and civil society organizations to use ICT tools in increasing public awareness on government issues, especially related to health, as well as potential solutions. iParticipate trains NGOs and journalists to conduct more data-driven analyses of the government information so that they can use these skills to advocate for public service reform, with the view that ordinary Ugandans will enjoy better services in the future.
Initiation of the open data activity
In 2011, the Collaboration on International ICT Policy for East and Southern Africa (CIPESA), a technology for development NGO, began promoting the use of ICT in monitoring good governance and service delivery in Uganda. The project, called Catalyzing Civic Participation and Democracy Monitoring Using ICTs, was funded by the Swedish Program for ICT in Developing Regions (SPIDER), a development resource center.25 It established partnerships with three grassroots-based organizations, namely, the Busoga Rural Open Source and Development Initiative (BROSDI) in the Mayuge district (Eastern Uganda); the e-Society Resource Centre (eSRC) in the Kasese district (Western Uganda); and the Northern Uganda Media Club (NUMEC), in Gulu (Northern Uganda). These organizations had been working directly with communities to promote the use of ICTs as tools for citizens to engage with decision-makers and demand accountability. Under their projects, citizens used various tools in engaging with local government officials, including radio (NUMEC), email, blogs, social media (BROSDI), and geo-coded mapping for eSRC.
Informed by the experience and networks developed by CIPESA through these previous efforts, iParticipate, the project under study here, sought to support these existing efforts and to build on them by leveraging open government data (much of it already available in various portals but often in incompatible or inaccessible formats) as an enabler of citizen participation and accountable governance, focusing especially on the health sector. CIPESA’s interest in open governance started when it conducted research on open governance network building in Uganda, funded by the International Development Research Center in 2012.26 Among other results, the research helped identify key datasets that citizen groups would like the government to proactively disclose, as well as the general level of government readiness to implement open governance in the country.
Much of the work undertaken under the iParticipate initiative focused on training intermediaries – particularly media and civil society actors – to enable and promote citizen participation in Ugandan governance. iParticipate also provided support to grassroots citizen-focused ICT centres like eSRC in Kasese. Finally, the project engaged with government officials and policymakers to help communicate the opportunities, tools and tenets of open data and open governance processes to push forward the supply side of open data and ensure that the institutional culture acted as an enabler of greater participation in governance and service delivery.27 This multi-audience focus helped iParticipate to diversify its offerings, engage relevant stakeholders in a targeted way, and avoid the “if you build it, will they come” question that often plagues open data efforts focused solely on citizens with little attention paid to intermediaries or actors on the supply side.
As explained further below, iParticipate provides detailed GIS-maps and visualizations to present mashed up datasets from a number of government data sources, in the process making clear where, how and why health care resources are being used across the country. Much of the project’s offerings are real-world rather than digital. iParticipate efforts have included, for example, multi-stakeholder meetings between government officials and educators focused on the challenge of implementing tools to improve community participation.28 Traditional media outlets are also leveraged – including through the previously mentioned radio broadcasts. The effort also involves the use of a number of training and engagement centers, including the eSRC in Kasese, which “provides ICT training programmes…aimed at enhancing citizens’ competence in monitoring government services, promoting accountability, civic participation and good governance.”29
One specific initiative undertaken in collaboration with NUMEC aimed at making government information more accessible to citizens in the districts of Gulu, Nwoya and Amuru – the regions most affected by Lord’s Resistance Army’s (LRA) destruction. The project set out to “document service delivery failures as a result of donor aid cuts to the Peace, Recovery and Development Plan (PRDP), and to generate debate by citizens through community debates, radio talk shows and ICT-based engagements on improving service delivery needs of post-conflict communities.” The PRDP was launched by the government in 2009 to “revitalise the economy and livelihoods of communities in the post-conflict region” through health service delivery, new infrastructure, clean energy and education initiatives, but widespread allegations of corruption destroyed citizen trust in the effort.30
The project’s overarching goal was to increase citizen participation in monitoring government service delivery through the use of ICT; advocate for government stakeholders to practice open governance; and document and propagate to the wider public the results of these processes. CIPESA performs the role of an intermediary that gathers government data and translates it into useful, relevant, and meaningful information for citizens. CIPESA’s aim is also to increase the capacity and ability of citizen groups and the media to demand better data, and to use this data to exact accountability from governments, especially in the health and education sectors.
Funding
The Swedish Program for ICT in Developing Regions (SPIDER) provided CIPESA with 500,000 SEK (approximately 55,480 USD) for a two-year implementation beginning 2013. The project from which this new initiative was built was also supported by SPIDER at the same funding level. In addition, Indigo Trust also provided 12,000 GBP (14,870 USD) for the initiative.
Demand and Supply of Data type(s) and sources
iParticipate’s health advocacy was focused on health service delivery and how access to health care, especially by the poor and marginalized in rural areas, is affected by government investments in people and facilities. There were a few primary data sets that were used by CIPESA in this process—those related to health clinics, health centers, and general hospitals, including the location and number of beds for each of these facilities. This existing data originated on the Ministry of Health website and was made accessible through Uganda’s Open Data for Africa portal.31
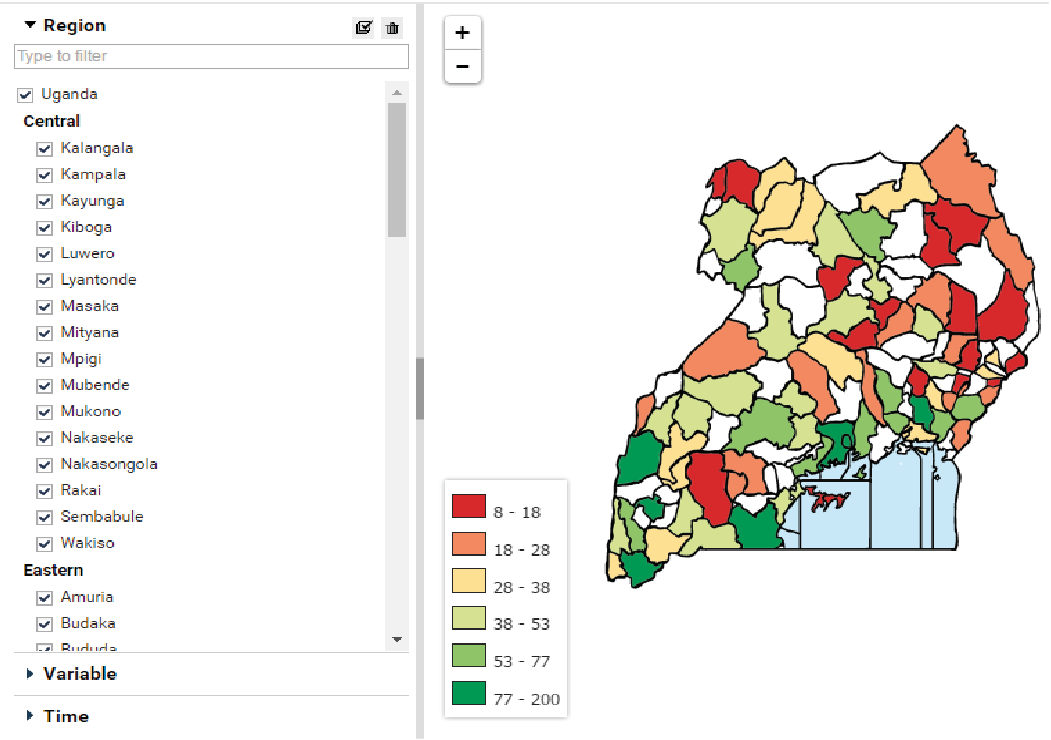
Figure 1. Location of hospitals, health clinics in Uganda (Source: Uganda Open Data for Africa Portal)
The Open Data for Africa portal allowed for online search and query, with the capacity to filter and visualize results (see Figure 1). The platform also allows downloading of data as CSV, XLS, or OData files. Similar datasets are also available at the Electronic Health Management Information System (eHMIS),32 though this portal requires formal log-on procedures to be able to get access to the data.
To see investments in health per jurisdiction, CIPESA used budget data from the Ministry of Finance Planning and Economic Development available at the ministry’s budget portal.33 The portal has an elaborate query facility and also publishes PDF reports of spending performance for each sector. Access to the data, however, is not fully open, as it requires registration with the data providers, and acceptance of registration is not assured.
Open Data Use
CIPESA used the data available in these portals and from other sources to analyze health service delivery and public investments in health projects. Much of iParticipate’s training efforts, for example, focused on providing individuals and journalists with the capacity to access and use geocoded maps made possible by open government data.
CIPESA used data to identify a number of features related to health service delivery. For example, iParticipate’s maps could help identify populations with limited access to health care, as well those health facilities that had limited or no beds. This information was cross-tabulated with funding information. As a result, iParticipate was able to show the need for more data sharing at all levels of the health service delivery infrastructure in Uganda. As Lillian Kisembo, the Assistant Town Clerk in Kasese, put it: “If we can embark upon sharing information at the local level, we can reduce these challenges at District planning.”34
In addition, CIPESA also made use of open data coming from different sources to build a platform to show how projects implemented through the PRDP, described above, collect reports coming from the field through users with Android phones, and aggregate different reports on health issues and health-related information. Community residents can report information using the Ushaidi35 crowdsourced mapping application and this, together with different reports and information, are consolidated in a crowd-mapping portal (see Figure 3).36
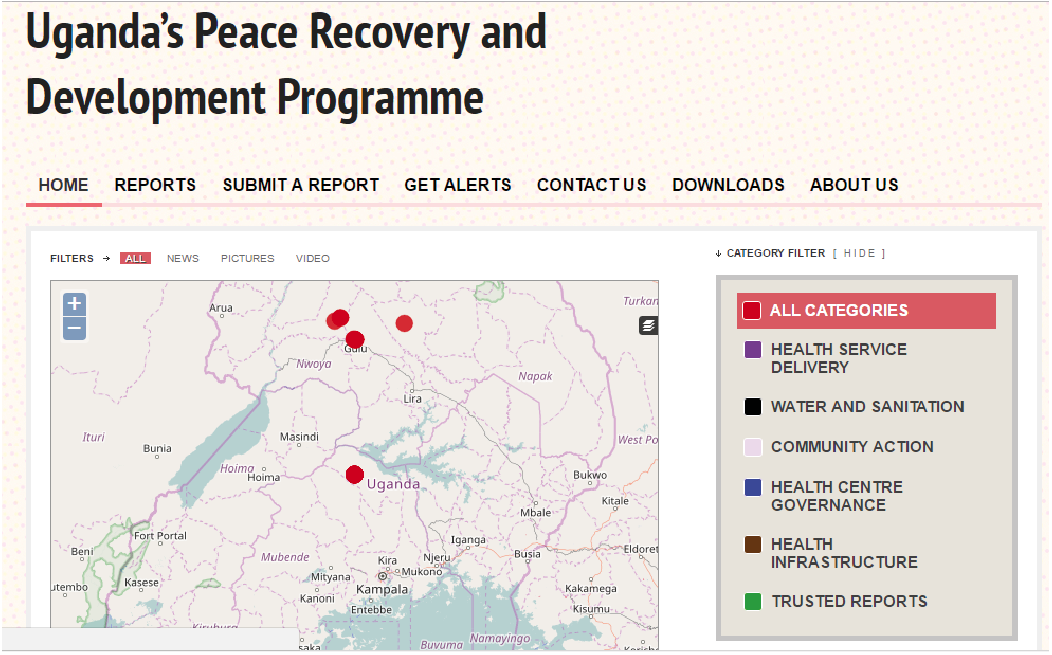
Figure 3. Crowd-mapping Platform developed by CIPESA - PRDP
Read MoreReference
1 . Project conducted in collaboration with the Web Foundation, United States Agency for International Development (USAID), and the Mobile Solutions, Technical Assistance and Research (mSTAR) program at FHI 360.
2 Special thanks to Akash Kapur who provided crucial editorial support for this case study, and to the peer reviewers who provided input on a pre-published draft.
3 . Swedish Program for ICT in Developing Regions website, http://spidercenter.org/. .
4 . African Health Observatory, “Comprehensive Analytical Profile: Uganda,” WHO, http://www.aho.afro.who.int/profiles_information/index.php/Uganda:Index.
5 . African Health Observatory, “Uganda: Factsheets of health statistics, 2016,” http://www.aho.afro.who.int/profiles_information/images/f/fb/Uganda-Statistical_Factsheet.pdf.
6 . AVERT, “HIV and AIDS in Uganda,” http://www.avert.org/professionals/hiv-around-world/sub-saharan-africa/uganda.
7 . Merlin L. Willcox, et al., “Human Resources for Primary Health Care in sub-Saharan Africa: Progress or Stagnation?” Human Resources for Health, 13, 2015, https://human-resources-health.biomedcentral.com/articles/10.1186/s12960-015-0073-8.
8 . Simon Peter Ogwang, “Fighting Corruption, Empowering People in Uganda’s Health Service,” Transparency International Blog, July 11, 2012, http://blog.transparency.org/2012/07/11/community-empowerment-in-uganda-using-icts-for-better-health-service-delivery/.
9 . Act!onaid, Corruption and the Service Delivery Tragedy in Uganda: Stories from the eastern leg of the anti-corruption caravan, Act!onaid, September 2014, http://www.actionaid.org/sites/files/actionaid/anti-corruption_report.pdf.
10 . Jeremy I. Schwartz, et al., “Toward Reframing Health Service Delivery in Uganda: The Uganda initiative for integrated management of non-communicable diseases,”Global Health Action, 8, 2015, http://www.globalhealthaction.net/index.php/gha/article/view/26537.
11 . African Health Observatory, “Uganda: Health information, research, evidence and knowledge,” WHO, http://www.aho.afro.who.int/profiles_information/index.php/Uganda:Health_information,_research,_evidence_and_knowledge.
12 . Ministry of Health, Republic of Uganda website, http://www.health.go.ug/.
13 . Opendata Barometer, “Rankings and Data: Uganda,” http://opendatabarometer.org/data-explorer/?_year=2015&indicator=ODB&open=UGA .
14 . World Bank, Open Data Readiness Assessment: Uganda, World Bank, http://opendatatoolkit.worldbank.org/docs/odra/odra_uganda.pdf
15 . Development Research and Training, Unlockiing the Potential of a More Harnessed Partnership among Open Data Actors in Uganda, Indigo Trust, November 2015, https://indigotrust.files.wordpress.com/2016/02/drt-indigo-trust-uganda-final-report.pdf.
16 . African Health Observatory, “Uganda: Health information, research, evidence and knowledge, analytical summary,” WHO, http://www.aho.afro.who.int/profiles_information/index.php/Uganda:Health_information,_research,_evidence_and_knowledge#Analytical_summary.
17 . Ministry of Health, Republic of Uganda website, http://hmis2.health.go.ug/#/
18 . African Health Observatory, “Uganda: Overview of the Flows of Information,” WHO, http://www.aho.afro.who.int/profiles_information/index.php/Uganda:Overview_of_the_flows_of_information
19 . Vincent Michael Kiberu, et al., “Strengthening District-based Health Reporting through the District Health Management Information Software System: The Ugandan experience,” BMC Medical Informatics and Decision Making, 14, 2014, http://bmcmedinformdecismak.biomedcentral.com/articles/10.1186/1472-6947-14-40.
20 . Human Resources for Health Information Systems website, http://hris.health.go.ug/reports/.
21 . Jillian Larsen, Uganda: Winning human resources for health, International Budget Partnership, December 2015, http://www.internationalbudget.org/wp-content/uploads/case-study-full-uganda-human-resources-for-health-2015.pdf.
22 . Collaboration on International ICT Policy in East and Southern Africa (CIPESA) website, http://cipesa.org/about-us/.
23 . Swedish Program for ICT in Developing Regions website, http://spidercenter.org/.
24 “CIPESA,” Promoting Human Rights and Democracy Through ICT, http://ict4democracy.org/about/partnerproject-briefs/cipesa/.
25 . Ibid.
26 “Uganda Open Government Data Readiness Study,” CIPESA and Association for Progressive Communications, April 2012, http://cipesa.org/?wpfb_dl=139.
27 “2015 Projects,” CIPESA, http://cipesa.org/projects/.
28 Caroline Wamala Larsson, “SPIDER Stories 2013-2014,” SPIDER Center, 2015, http://spidercenter.org/wp-content/blogs.dir/362/files/2016/11/spider_stories_2013-2014_for_web.pdf.
29 Ashnah Kalemera, “Citizens’ Use of ICTs in Social Accountability in Uganda’s Kasese District,” CIPESA, January 19, 2015, http://cipesa.org/2015/01/citizens-use-of-icts-in-social-accountability-in-ugandas-kasese-district/.
30 Gladys Oroma, Promoting Communit Dialogue on Service Delivery Failures in Northern Uganda,” Promoting Human Rights and Democracy through ICT, February 28, 2015, http://ict4democracy.org/promoting-community-dialogue-on-service-delivery-failures-in-northern-uganda/.
31 . Open Data for Africa, “Uganda Regional Health Statistics Database, 2011,” http://uganda.opendataforafrica.org/lhcqofd/uganda-regional-health-statistics-database-2011
32 . Ministry of Health, Republic of Uganda website, http://hmis2.health.go.ug/#/.
33 . Ministry of Finance Planning and Economic Development, “Uganda Budget Information,” http://budget.go.ug/index.php?p=budget_dashboard.
34 “ICT4Democracy in East Africa: A Year in Review 2015,” CIPESA, 2016, http://cipesa.org/?wpfb_dl=221.
35 . Ushahidi website, https://www.ushahidi.com/.
36 . CIPESA, “Promoting Transparency, Civic Agency and the Right to Information in Northern Uganda’s Peace Recovery and Development Programme,” https://cipesa.crowdmap.com/main.
37 . CIPESA, ICT in Civic Participation and Democracy in Uganda: Citizens’ knowledge, attitudes and practices, CIPESA ICT Policy Research Series, No. 4/15, 2015, http://www.cipesa.org/?wpfb_dl=196
38 . Ibid.

